Lokarpit Voice: How Does It Work?
We have been developing and test-deploying a "voice forum." In its simplest form, one may think of it as a web-enabled voice mail system and a voice database. The villagers that we serve access the system with their regular voice phones. (In our experience, virtually all of those who don't have their own phones have access to someone else's.) The villagers can leave their personal queries, receive personal responses (that address their specific concerns), or receive broadcast messages (that are of interest to larger groups). For those who have access to more sophisticated technologies, such as staff, nurses, doctors and some of the trainers, the voice system is accessible via a web database interface. The incoming messages are categorized, filtered, and assigned to groups of potential responders. Those who choose to respond or are tasked to respond may submit answers via either the web interface or their own cell phones. The responses are then sent at their preferred times back to the villagers who made the initial queries.
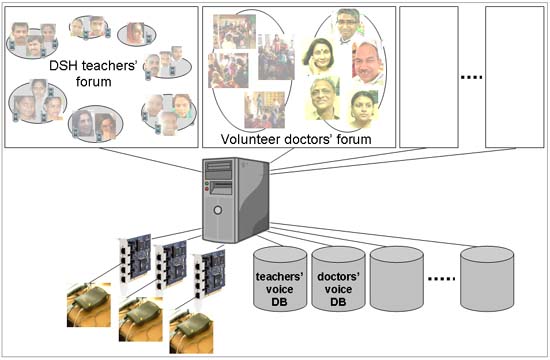
Voice mail systems are obviously not new. We discuss how our system is technically and functionally innovative. Traditionally, such an application (such as the well-regarded "Lifelines" system) is typically developed with expensive and proprietary PBX equipment and software, often with the blessing of carriers. The traditional approach is costly, difficult to customize, and difficult to justify for small groups of targeted users. The carriers' main interest is a large-scale one-size-fits-all system that can earn non-trivial revenue and can be administered centrally. In contrast, our system is built on top of cheap ISDN line cards plugged into conventional PCs and the open-source Asterisk framework. (The voice servers simply sit in our regional offices, as opposed to being inside telecom carriers' machine room closets.) The decentralized development and deployment is low-cost, provides extreme ease of local customization, and makes it feasible for us to experiment with tailor-made solutions for small local populations and experts. The solution can be easily and cheaply replicated at many locations, and because these distributed systems are networked, the information can be easily shared across the entire network of voice servers.

Functionally, the system that we have built is much more than a voice mail system. A vanilla voice system mostly just provides one-to-one exchanges. In our system, on the other hand, for example, an exchange between a villager and a nurse is stored in a voice database, and if deemed appropriate (and with proper privacy precautions), the same exchange can be either re-used for another villager or re-broadcast to an even larger group (such as an interest group created for pregnancy or child nutrition). Indeed, one extra outlet of the voice database is community radio systems, which can be enlisted to beam frequently asked questions and answers to selected communities. (We are also building and experimenting with "phone radio boxes," boxes that behave like radios but receive their programming from cellphone links and can be interactive.) Furthermore, as discussed above, voice data initially gathered at one locale can be shared with other peer networked voice servers serving other locations. The knowledge accumulation in such a voice database and the strategic re-use of the information is critical in addressing the "expert bandwidth" problem.

Another area of our innovation that lies somewhere in between low-level underlying technology and high-level functionality is usability. For example, we have found that for some of our poorest areas, even the cost incurred during the making of a cellphone call is a non-trivial burden. Our solution is that our system can be programmed to automatically dial villagers who have signed up to participate in our system and have specified at which times they prefer to receive calls (once a week, for example), and at these preferred times they can record their new queries or concerns and hear new messages intended for them. (Receiving calls is free in India.) We have found that our users' ability to specify their preferred times of receiving automated calls is critical. This example is but one of the many usability issues that we have worked on to make our system easier for our users to participate in.

An important functionality of this networked voice forum is that it allows potential contributers to work together in an easy and flexible way. For example, in addition to doctors who work in our target areas, potential contributers elsewhere, such as medical school students and even professionals working in the US, can easily listen to queries submitted from rural Uttar Pradesh and submit their own responses. The language problem can be overcome when volunteer translators, who possess no special medical knowledge, transcribe voice submissions and record newly translated outgoing responses through the system. Healthcare workers who possess less specialized knowledge can at least perform duties such as categorizing and sorting incoming messages and assigning them to the right kinds of potential responders who have more specialized knowledge. This division of responsibilities and the ability of people with diverse skills to work together, across potentially widely separated space and time, is a powerful force multiplier.

Of course, the role of the system should be largely informational, not "playing doctor" in emergency situations--we fully recognize that we cannot expect to cure people over just a voice mail system. The hope is that by making access to health information much easier, we can catch milder problems before they develop into emergencies, and in cases of real emergencies, the best we can do is to advise seeking in-person care at a clinic or hospital as soon as possible. In the future, we plan to tie the voice forum to existing physical activities, such as regular "camp runs" of van visits staffed by doctors and nurses from participating local hospitals and clinics.

Let us also briefly discuss how the other challenges (discussed earlier) facing traditional maternal health awareness projects are addressed by the proposed system. The fidelity loss problem of traditional cascaded training model is addressed by the voice forum's ability of directly connecting questioners and expert answerers. In addition, the voice forum database itself can become a good training tool, as mid-level responders can increasingly familiarize themselves with the types of questions and expert answers being exchanged, so that they become increasingly capable of "filtering" the questions first, further reducing the burden on the experts whose times are most valuable.

The need to avoid relying too much on traditional one-size-fits-all broadcasts (including approaches like distributing brochures) that cannot effectively address diverse local customs and concerns is addressed by the fact that the information exchange in our voice forum is on the one hand driven by real-life queries from villagers, and is on the other hand driven by professionals with the greatest local practice experience. (Our system also allows discussions of important issues that are not strictly health-related, such as women's rights, alcohol abuse (by husbands), and girl child's education.)

The need to avoid using complex and expensive technologies that are inappropriate for a largely illiterate population is addressed by the fact that the only equipment the villagers would need to access our system is simple voice phones. Furthermore, the underlying technology powering the voice servers is such that the infrastructure serving the voice forum can be scaled cheaply, easily and gradually (if necessary). Our hope is that one day, we will be running a large network of these voice servers, buzzing 24 hours a day with queries and answers coming into the system from everywhere, ranging from villagers of the remotest locales to professionals from the most prestigious institutions, constantly serving a large population that need help the most.
For more information, here is a write-up. Here are some slides.